

Hip Pain In Athletes: Understanding Femoral Anterior Glide Syndrome
Hip pain – particularly of the anterior (front of the hip) variety – is a very common problem in the weight training population.
In her book, Diagnosis and Treatment of Movement Impairment Syndromes, Shirley Sahrmann discusses Femoral Anterior Glide Syndrome in excellent detail. And, while it may seem like an obscure diagnosis, it’s actually a really common inefficiency we see in a weight training population.
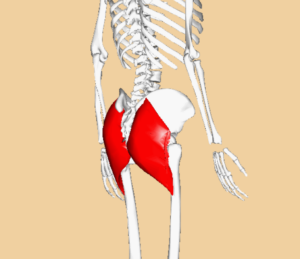
In order to understand this syndrome, you have to appreciate the attachment points and functions of the hamstrings and gluteus maximus. With the hamstrings, you’ll notice that they attach to the ischial tuberosity of the pelvis (with the exception of the short head of the biceps femoris, which attaches on the femur), and then run down to a point inferior to (below) the knee. In other words, they are a two-joint muscle group. All of the hamstrings aid in knee flexion, and all but the short head of the biceps femoris also aid in hip extension.

Conversely, the glutes attach on the pelvis and the femur; they’re a one-joint muscle – and this is why they can so directly impact hip health.
You see, when the hamstrings extend the hip (imagine the hip motion that happens when one comes out of the bottom of a squat), they do so in a “gross” fashion. In other words, the entire leg extends. In the process, there is little control over the movement of the femoral head (“ball” in the “ball-and-socket” hip joint) – and it tends to migrate forward during hip extension, giving you a femoral anterior glide syndrome. In the process, it can irritate the anterior joint capsule, and this irritation can give a sensation of tightness in the front of the hip.
Fortunately, the glutes can help prevent the problem. Thanks to their point of attachment on the superior aspect of the femur (closer to the hip), they have more direct control over the femur as it extends on the hip. As a result, they can posteriorly pull the femoral head during hip extension. So, in an ideal world, you get effective co-contraction of the hamstrings and glutes as one extends the hip; they are a system of checks and balances on one another. If you use the hamstrings too much in hip extension, you’re just waiting to develop not only femoral anterior glide syndrome, but also hamstrings and adductor magnus (groin) strains and extension-based back pain.
As an aside, this hamstrings/glutes relationship is somewhat analogous to what you see at the shoulder with the subscapularis posteriorly pulling the humeral head as the infraspinatus and teres minor allow it to drift forward. That’s another newsletter altogether, though!
Once the femoral anterior glide issue is in place, the first course of action is to stop aggressively stretching the hip flexors. While the issue gives a sensation of hip flexor “tightness,” in reality, stretching the area only exacerbates the anterior hip pain. A better bet is to just ditch the stretching for a few days, and instead incorporate extra glute activation work. Eventually, though, one can reintegrate both static and dynamic hip flexor stretches.
Just as importantly, it’s important to identify the causes. We’ll see this issue in runners who have no glute function, but more commonly, I’ll see it in a weight training population that doesn’t understand how to complete hip extension. Here’s what a hamstrings-dominant hip extension pattern would look like with squatting.
The final portion of hip extension is when the glutes are most active, so it’s important to “pop the hips through” at lockout of deadlifts, squats, pull-throughs, and other exercises like these. In the same squat example, it’s really just as simple as standing tall:
Of course, this is just the tip of the iceberg when it comes to hip issues in athletes, but it’s definitely something we see quite a bit. If you’d like to learn more, I’d highly recommend you check out our Functional Stability Training series, particularly the Lower Body and Optimizing Movement editions. They’re on sale for 25% off through tonight (Cyber Monday) at midnight.
Enter your email below to subscribe to our FREE newsletter and you’ll receive a detailed video tutorial on how to deadlift!
Archives:

