

3 Random Thoughts on Rotator Cuff Readiness
Both Cressey Sports Performance facilities are booming with baseball players coming back to start their offseason training, so it’s the time of year when athletes are working hard to get their rotator cuff control back before they start up their offseason throwing programs. With that said, I’ve been thinking about some big principles on the rotator cuff readiness front.
1. In a broad sense, just about every rotator cuff exercise can be categorized in one of five ways:
a. Strength – this consists of manual resistance work and anything with cables at dumbbells; it needs to be loaded up and challenging.
b. Timing – this consists of drills like 90/90 holds and rhythmic stabilizations.
c. Endurance – this builds on what we see in Option A (some of the same exercises), but the resistance is a bit lower and it’s done for higher reps or a longer time. The goal is less about strength and more about training the ability to hold the humeral head on the glenoid fossa for a lengthier period of time. I’d call it more important for a sport like swimming than for baseball or tennis athletes.
d. Irradiation – this can refer to just about any exercise, as your rotator cuff fires reflexively any time your arm moves. That said, certain exercises – bottoms-up kettlebell variations, for instance – are particularly useful for challenging this category of drills.
e. Patterning – these are just drills that take the humerus through its full range-of-motion. Of particular importance is end-range external rotation, which we train with drills like this:
2. I prefer near-daily exposures rather than exhaustive, less frequent programs.
If you look at our training programs, most of our pro guys are doing some kind of targeted training for the rotator cuff 5-6 days per week. Twice per week, we’ll push more strength and irradiation work, and twice per week, we’ll cover more timing drills. Just about every day, though, there will be some kind of patterning exercise so that we’re reminding the cuff of what it’s supposed to do.
This approach is a stark contrast to what you usually see in the baseball world, which is notorious for handing out the 2x/week arm care routines that take 45-60 minutes each. They’re usually about 15 exercises for multiple sets, and leave an athlete hanging by the end of the session. I think this approach has more to do with the fact that it lines up with what’s convenient for 2-3x/week physical therapy sessions than because it’s truly optimal. I’m of the belief that you don’t need (or want) to exhaust the cuff to get it to where it needs to be.
And, while we’re at it, if the cuff is going to get abused on a daily basis with throwing, lifting, and activities of daily living, why not give it some more frequent exposure to build a little tissue resiliency?
3. Posterior deltoid shouldn’t be lumped in with infraspinatus and teres minor.
Many times, the reason we have discomfort or the “wrong” feeling with drills is that athletes are paying close attention to the osteokinematics – gross movements of internal/external rotation, flexion/extension, adduction/abduction – of the joint in question, but not paying attention to the arthrokinematics of that same joint. In other words, the rolling, rocking, and gliding taking place needs to be controlled within a tight window to ensure ideal movement.
In shoulder external rotation variations, as we externally rotate the arm, the humeral head (ball) likes to glide forward on the glenoid fossa (socket). The glenohumeral ligaments (anterior shoulder capsule), rotator cuff, and biceps tendon are the only things that can hold it in the socket. In a throwing population, the capsule is usually a bit loose and the cuff is a bit weak, so the biceps tendon often has to pick up the slack – which is why some folks wind up feeling these in the front, thereby strengthening a bad pattern. There are also a bunch of nerves at the front of the shoulder that can get irritated.
Now, here’s where things get a bit more complex. The infraspinatus and teres minor are both rotator cuff muscles that have attachments right on the humeral head, so they can control the arthrokinematics (posterior glide) during external rotation work. Conversely, the posterior deltoid (blue, in the image below) runs from the posterior aspect of the spine of the scapula to further down the arm on the deltoid tubercle. In other words, it completely bypasses control of the humeral head.
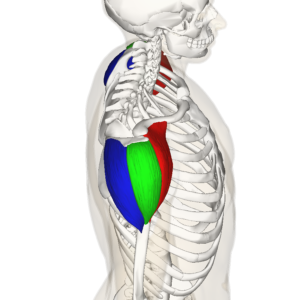
By Anatomography – en:Anatomography (setting page of this image), CC BY-SA 2.1 jp, https://commons.wikimedia.org/w/index.php?curid=22835985
With this in mind, the posterior deltoid actually creates a gliding forward of the humeral head as it externally rotates and horizontally abducts the arm. For this reason, you need to make sure the arm doesn’t come back (horizontal abduction) as it externally rotates during your arm care drills. This video should clarify things, if you’re a visual learner:
Looking for more insights like these? Be sure to check out my new resource, Sturdy Shoulder Solutions.

Archives:

