

Pitching Injuries: Should Lat Strains Even Be Happening?
In a 2016 meta-analysis, researchers examined the existing body of research on latissimus dorsi and teres major strains in professional baseball pitchers. While the collective sample size was small (30 total athletes), one resounding theme was present:
Lat strains can be pain in the butt to rehabilitate.
In these studies, 29 pitchers were managed conservatively, while one pitcher required surgery for the issue. In the conservative group, the average return-to-pitching timeline was 100 days, whereas the surgical case was 140 days.” Perhaps of more significance, though, the researchers noted that “five patients in the conservative group suffered from complications and/or setbacks during their treatment and rehabilitation.”
We have to keep the sample sizes in these studies in mind, too. They haven’t had a large pool from which to draw, and many researchers might not appreciate how different “return-to-pitching” is than “feeling like your old self.” The general consensus among guys I know who have had the surgery seems to be that it’s 8-10 months before you’re back to feeling 100% in games.
Let’s face it: if you’re missing 3.5-5 months with an injury – and adding even more time to get back to 100% – you might as well just cash in an entire season. That’s not only a lot of money wasted on disabled list time at the Major League level, but also a lot of lost developmental time in the minor league ranks.
To make matters worse, the rehabilitation process can be delayed because lat strain diagnoses can be somewhat challenging. According to Dr. Leon Scott, a sports medicine physician and Assistant Professor of Orthopaedics & Rehabilitation at Vanderbilt University, “Because lat strain diagnoses aren’t all that simple to make, especially if a physician’s exam is limited and relies heavily on an MRI, they are often a missed diagnosis. A standard MRI may not be distal enough to capture the area of injury. Arthrogram images are an even smaller field, leading to a missed diagnosis.” He also notes that in one acute lat injury he saw in the past, “With a wide field shoulder MRI, there was acute edema, hematoma seen at the bone-tendon interface. It was hard to miss.” In short, ordering physicians may be trying to use a narrow imaging technique for a shoulder injury when they should be painting with a broader brush that would also pick up an upper arm injury.
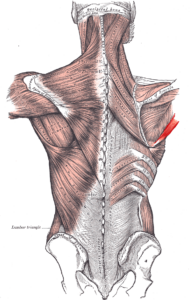
Source: By Anatomography (en:Anatomography (setting page of this image)) [CC BY-SA 2.1 jp (https://creativecommons.org/licenses/by-sa/2.1/jp/deed.en)], via Wikimedia Commons
One professional player I saw struggled with getting a definitive diagnosis that his lat strain needed surgery for two years. At first, they suspected his anterior shoulder pain was occurring because of a labral tear, but a labral “clean-up” surgery didn’t change his symptoms. Perhaps more interesting, though, the surgeon didn’t even see the lat tear while he was doing the arthroscopic intervention. Five months later, another surgeon went in to repair the lat – which was actually significantly detached from the bone.
The first take-home message here is that if you’re a thrower and you have shoulder pain, you need to make sure that you see a sports medicine physician who sees a lot of throwing injuries. A lat strain can be a tricky diagnosis, and even the most well-intentioned physicians may not know to look for it. This is especially because it often presents as pain in the front of the shoulder, in the event of a tendinous injury. You can see this clearly demonstrated by the attachment points in the image above, but I’ll take more about this later when we get to functional anatomy.
As I pondered the research article and actually discussed it with a few of my staff members, I realized that we have literally never had a lat strain happen with one of our regular clients at Cressey Sports Performance – and we see a lot of pitchers. I say this not to brag (or jinx us), but rather to just bring to light that success leaves clues – which I’ll also get to later on in this article.
That said, I should note that my ideas in this article also draw heavily on our experiences working with a lot of frustrated pitchers who have come to work with us after the injury has occurred because they need help bouncing back. Failures (in this case, injuries) also leave clues.
Before we get to all these observations and potential countermeasures to prevent lat strains, I think it’s incredibly important to discuss the functional anatomy of the latissimus dorsi and teres major. And, as an extension, we’ll discuss how this functional anatomy understanding needs to be put alongside biomechanics research and anecdotal observations of injured athletes to pull together a hypothesis for the “perfect storm” of lat injury risk.
Functional Anatomy
The latissimus dorsi is a big muscle with huge functional implications.

It attaches on the thoracolumbar fascia (lower back) and runs all the way up to the intertubercular groove of the humerus (front of the upper arm). This is why it has to be considered as a differential diagnosis for anterior shoulder pain in throwers – alongside everything from biceps and rotator cuff tendinopathy or tears, to labral injuries, to anterior capsule injuries, to thoracic outlet syndrome.
As an interesting aside, there are a number of anatomical variants present along this lengthy anatomical course. In a small percentage of people, the lat actually attaches on the ilium (top of the pelvis). In just under half of individuals, it has a direct attachment on the scapula. The number of costal (rib) and vertebral attachments also varies from person to person.
Everyone knows about the functions of the lat at the shoulder – extension, adduction, internal rotation, and horizontal abduction – but in consideration of this expansive functional anatomy profile, we have to appreciate that it has several other key roles to consider.
Lat is a key core stabilizer – to the point that it can be heavily overused and pull athletes into a “gross extension” pattern. Notice the big anterior pelvis tilt and lordosis here – but also take note of the position of humeral extension (and the indirect effects on forward head posture).

Given its attachment on the scapula in some individuals – and the indirect impacts of “crossing” the scapular region – the lat also contributes to scapular depression.

Finally, it’s been theorized that an aberrant, extension-biased posture would interfere with optimal diaphragmatic function (via loss of the zone of apposition). Because the lat is also an accessory respiratory (inhalation) muscle, you could say that it has to pick up the slack for a problem it actually helps create! My favorable experiences with the Postural Restoration Institute and my own anecdotal observations definitely support this theory.

Source: www.PosturalRestoration.com
For all intents and purposes, you can view teres major as a “mini-lat.” It shares the same scapula-to-humerus functional relationship and actions, but doesn’t impact the rib cage or lumbar spine directly.
Implications for Throwers
By appreciating the functional anatomy of the lat, we can recognize just how vital it is to throwing a baseball hard. In short, it connects the lower body to the upper body to allow for force transfer that ultimately leads to arm speed and ball velocity.
Not surprisingly, a 1987 study from Gowan et al. observed that lat recruitment during the acceleration phase of throwing was substantially higher in professional pitchers than in amateurs. Not surprisingly, experienced, accomplished athletes know how to use big-boy muscles (prime movers) to do big-boy jobs (accelerate the arm, which is the fastest motion in all of sports). The amateur pitchers actually continued to heavily rely on smaller, stabilizing muscles – the rotator cuff, biceps, and posterior deltoid – during acceleration. That’s not a safe or effective long-term strategy.
This is likely why we rarely see lat strains in younger athletes; you probably have to throw 90mph+ to effectively “use” the lat, and muscles that don’t get used usually don’t get strained. The younger kids are more likely to have rotator cuff pain, irritation of the long head of the biceps tendon, or proximal humeral growth plate issues.
There’s a bit more to “lat overuse” than just the acceleration phase of throwing, though. During the lay-back (extreme cocking, or maximum external rotation) portion of throwing, the lat and teres major are two of several muscles (including notables like subscapularis pectoralis major) that are working eccentrically to prevent the humerus (upper arm) from flying off the body.

This eccentric pre-stretch also helps to store elastic energy that is subsequently released during the acceleration phase to create ball velocity. Most muscle strains occur – whether it’s acutely or chronically – as muscles and tendons are stretched during the eccentric phase of activity. Hamstrings strains usually occur at the terminal swing phase of sprinting. Middle-aged men rupture Achilles tendons when they land on dorsiflexed ankles – where the calves are maximally stretched. The lats and teres major are the most overstretched at this lay-back phase of throwing.
On a chronic note, repeated exposures to aggressive eccentric stress can lead to muscle shortening. Reinold et al (2012) demonstrated this with respect to elbow extension and shoulder internal rotation. My experience has been that pitchers who trend toward the “tight” end of the continuum also lose shoulder flexion and “true” external rotation over the course of the season. As I describe in the video below, this is very likely related to stiffness or shortness in the lats – and the research has demonstrated that it is associated with an increased risk of elbow injuries in pitchers.
Beyond just the specific roles of the lats during the throwing motion, we have to also appreciate that they’re heavily overused during daily life because of their roles as core stabilizers and accessory respiratory muscles. And, given that we don’t spend a lot of time in our daily lives with our arms overhead and shoulders externally rotated, they aren’t afforded a whole lot of length throughout the day. Take a chronically shortened muscle, overuse it, and then throw it into the fastest motion in all of sports, and you’ve got a recipe for strains. However, you can’t throw hard without it. Hence, this Tweet from me a few years ago:
Why Do These Injuries Take So Long to Heal?
Having established the injury mechanisms, it’s important to also consider why lat strains in throwers take so long to rehabilitate. I see four primary reasons that differentiate lat strains from just “any other muscle strain:”
First, as we noted earlier, early diagnosis may not happen. This can occur because the athlete just ignores the issue as normal soreness, or they manage it as “biceps tendonitis.” Or, a physician may not recognize that a lat injury could create anterior shoulder symptoms. Finally, a typical MRI might just miss the injury altogether. All these factors can potentially lead athletes down the wrong rehabilitation path.
Second, my experience has been that many of these injuries are far more chronic than they are traumatic. More often than not, when you dig deeper into the history of a pitcher who has a lat strain, he’s thrown through some kind of extended soreness/discomfort for weeks, months, or years. Eventually, it becomes too much to stand and begins to significantly interfere with pitching performance. Given that the issue developed over an extended period of time, it isn’t going to go away overnight.
Third, as I discussed in my functional anatomy musings earlier, the lats are heavily involved in multiple planes of motion. I’ve theorized in the past about how muscles that play crucial roles in multiple plans are more likely to be stubborn rehabilitation projects:
Pull a quad (rectus femoris), and you’ll usually bounce back really quickly. Pull an oblique and it’s much more stubborn. What’s the difference? The rectus femoris is really all about the sagittal plane, whereas the obliques have a big role in controlling excessive motion in the sagittal, frontal, and transverse planes. The more complex the job of the muscle, the more significant the injury – and the longer the rehab. Hamstrings have roles outside the sagittal plane and can be equally stubborn, too.
Fourth, the proximal humerus (upper arm) area really seems to scar down faster than almost any other region in the body – and this is particularly true of throwing shoulders because of the eccentric stress pitchers encounter. There are 17 muscles that attach to the scapula, and most of these structures cross the glenohumeral (ball-and-socket) joint. Perhaps more significantly, eight of these tendons attach in close proximity to the insertion of the latissimus dorsi and teres major. Throw eight tendons in a very small area that experiences a lot of eccentric stress, and you’ll wind up with a gritty, fibrotic mess eventually.
Injury Risks
Whether it’s a chronic or traumatic onset lat issue in a pitcher, one theme always seems to hold true: symptoms emerge after a dramatic increase in throwing stress.
On multiple occasions, I’ve seen lat strains that have come about because a reliever pitcher was moved into the starting rotation without a gradual increase in pitch count.
In other instances, the lat got cranky after a big velocity jump in a single off-season. This is usually the case in a high school kid who jumps from 84 to 94mph in a single winter. As my friend Derek Johnson, the pitching coach for the Milwaukee Brewers has said, the “arm is writing checks the butt can’t cash.”

Sometimes, it may come about after a single outing with an abnormally high pitch count. The pitcher just can’t bounce back in time for the next start, and the subsequent start becomes the straw that breaks the camel’s back. y experience has been that when you throw the typical “high arm speed” (90mph+) high school pitcher out for back-to-back outings of 100+ pitches – even on a seven-day rotation – things often start to head down the wrong path. This doesn’t happen nearly as frequently in the college game, and I think this speaks to the fact that there is clearly something really important that’s occurring in terms of work capacity and/or strength improvements for pitchers in the 16-19 age range.
Finally, lat issues seem to be particularly common when you see high school and college starters switch from a 7-day rotation to a 5-day rotation when they enter professional baseball. It isn’t as much of a dramatic increase in stress as it is a significant loss in recovery time or capacity. I’ve heard many guys over the years say that they have to learn to pitch with only 90% of what they’re typicaly capable.
Movement Quality
Beyond just the increase in throwing stress, there are a few things I’ve found to be common in the lat strain pitchers I’ve seen in recent years.
1. The lower traps can’t keep up with the lat.
The lower traps are very important for providing posterior tilt (slight tipping back) of the scapula and assisting in upward rotation. These two functions make it essential for a pitcher to get his scapula in the right position during the lay-back phase of throwing.
Conversely, the lat has more of a “gross” depression effect on the scapula; it pulls it down, but doesn’t contribute to posterior tilting or upward rotation. This might help with an adult rotator cuff pain patient who has an aggressive scapular elevation (shrug) substitution pattern, but it’s actually problematic for a thrower who is trying to get his scapula up and around the rib cage to make sure that the ball-on-socket congruency is “flush” when it really matters:
As such, you can say that the lat and lower trap “compete” for scapular control – and the lat has a big advantage because of its cross-sectional area and multiple attachment points. It’s also much easier to train and strengthen – even if it’s accidentally.
To this end, we’ll often hear throwers cued “down and back” during their arm care drills. The intention – improving posterior tilt via lower trap activation – is really good, but the outcome usually isn’t. Unless athletes are actually put in a position of posterior tilt where they can actually feel the lower traps working, they don’t get it. Instead, they pull further down into scapular depression, which feeds the lat-dominant strategy. This is why we teach almost all our throwers to differentiate between depression and posterior tilt on their first day in the gym.
2. The rotator cuff can’t keep up with the lat.
As I noted earlier, the lat has numerous functional roles at the shoulder. Because the attachment point of the lat is on the shaft of the humerus and not the ball, the lat really can’t have any direct control on the positioning of the ball in the socket. In fact, it actually indirectly destabilizes the throwing shoulder because it contributes to an anterior (forward) gliding of the ball on the socket during the lay-back phase of throwing. This anterior glide is counteracted by the rotator cuff musculature.
Whenever we evaluate movement, we have to consider both osteokinematics (gross movements – flexion, extension, etc. – of bones at joints) and arthrokinematics (subtle movements – rolling, rocking, gliding, etc. – of bones at joint surfaces).
To paraphrase something that physical therapist Shirley Sahrmann has noted many times, whenever you see a strained or overworked muscle, look for a dysfunctional synergist. In this case, the synergists to the lat and teres major are the rotator cuff muscles. We just rarely consider lat strains as a consequence of rotator cuff weakness because it’s usually the biceps tendon, labrum, capsule, or rotator cuff itself that winds up cranky before the lat starts barking.
3. Guys usually have a history of doing a lot of lat dominant lifting.
In a baseball population, throwing is lat dominant. Breathing is lat dominant. Core stabilization is lat dominant. When you add in a lot of lat dominant lifting to the mix – particularly during the in-season period – things don’t usually go well. I’m just going to put this out there:
[bctt tweet=”I’ve never met a high-level thrower who had weak lats.”]
I’m speaking with respect to both relative and absolute measures. Relatively speaking, I’ve never looked at a guy and said, “Well, if he added 50 pounds to his best weighted chin-up, he’d definitely throw harder and be healthier. His rotator cuff and lower traps are too strong.” Absolutely speaking, I have yet to see any research examining the relationship between lat strength and throwing velocity. I’m very confident that there is a point of diminishing returns where getting stronger doesn’t help add any more velocity. Moreover, it may actually interfere with improvements – and increase susceptibility to injury. This includes elbow irritation, as heavy weighted pull-ups and chin-ups are brutal on the medial elbow in lifters who don’t even throw a baseball for a living.
Just like you don’t have to squat 800 pounds to have an elite vertical jump – but you probably won’t jump high if you only squat 200 pounds – your lats just need to be strong enough to throw hard.
Also worthy of mention is the fact that exercises like deadlifts, farmer’s walks, and dumbbell lunges, and any other drill where weights are held in the hands are actually very lat intensive. With the arms at the sides, the lats are almost fully shortened – and the lat is working hard as a core stabilizer against appreciable external loading.
The take-home message is that you really have to critically examine your entire strength training program for how much lat-dominant work your athletes are doing. My rule of thumb is that an athlete has to have full shoulder flexion and great cuff strength to “earn the right” to do pull-ups in his off-season programming, and we don’t use any pull-ups or pulldowns with in-season programs. We can accomplish everything we need with horizontal pulling variations.
4. Guys usually accumulated a lot of innings or appearances without much, if any, manual therapy
NASCARs require more upkeep that ordinary automobiles. If you’re going to push a car to its limits, you better plan on changing the oil and tires more frequently. The same goes for a high level throwing arm. Manual therapy is a game-changer for maintaining or improving range-of-motion and bouncing back between outings.

The lats and teres major get pushed really hard during the throwing motion, and it’s important to do regular routine manual therapy maintenance to keep them “supple” with a variety of soft tissue approaches. I’ve seen athletes that responded really well to cupping, some to Graston Technique, some to Active Release Technique, some to dry needling, and others to more traditional massage. Everyone is different – but everyone needs it.
Also worth of note, trigger points in the latissimus dorsi may actually relate to discomfort in other regions. Chris Howard, massage therapist at Cressey Sports Performance – MA, notes:
“Trigger points in the latissimus dorsi can refer pain and discomfort to the medial and inferior border of the scapula extending to the posterior shoulder, medial triceps region and down to the pinky and ring finger. Trigger points not only cause pain, but can also mimic nerve symptoms by causing numbness and tingling in their referral zone. Of particular interest to this article is the fact that trigger points, regardless of whether they are active or latent, have the ability to alter muscle activation patterns. In other words, once trigger points are present in muscles of the shoulder girdle, the normal activation pattern is altered, which can lead to abuse of some of the smaller muscles.”
5. Guys have insufficient anterior core control.
The stiffer (or shorter) your lats are, the more you need to have great anterior (front) core control to prevent this from happening:
When the core control isn’t present, the lats are never really challenged to approach their end range – which is full shoulder flexion. Learning to add some good stiffness to lock the ribs to the pelvis during overhead motion obviously protects the lower back, but it also has the added benefit of making lats “healthier.”
6. They turn all rowing motions into lat dominant movements.
Rather than reinvent the wheel on this point, check out this detailed rowing technique video I filmed a while back. In particular, points #1, #2, #4, and #6 are the most common findings in a very lat-dominant individual. I’d encourage you to watch the entire video, though, as it’s not uncommon to see multiple mistakes at a time:
7. Guys have lost shoulder flexion.
If a muscle is fundamentally short, it’s going to be more likely to strain. These are usually the ones who have failed miserably on points 1-6 over an extended period of time.

Prevention
Several years ago, in the heart of the ACL prevention program craze, Mike Boyle made a bold statement, “ACL injury prevention is just good training.” In short, if you teach athletes to move well with comprehensive, well-rounded programming and solid coaching to ensure good training technique, you’re going to markedly reduce the incidence of ACL injuries. I couldn’t agree more – and I’d argue that lat strain prevention training in pitchers is just good training, too.
1. Maintain tissue quality with regular manual therapy, and complement it with daily foam rolling.
2. Make athletes earn the right to do pull-ups.
3. Don’t do pull-ups/pulldowns during the season.
4. Make sure that the rotator cuff, lower trap, and anterior core are strong enough to keep up with the lats.
5. Be cognizant of overdoing it on drills like deadlifts, farmers walks, and DB lunges/split squats. These are all great exercises that can have their place, but anything done to excess can be a problem.
6. Ensure appropriate training technique. Specifically, don’t overuse the lats when you aren’t supposed to use them at all.
7. Closely monitor athletes who have seen dramatic jumps in pitching velocity or workload – and avoid building up pitch counts too quickly.
8. Constantly solicit feedback from pitchers so that mild lat soreness is discovered before it can become a full blown injury.
Obviously, once an athlete already has a teres major or lat strain, things are a lot hairier. That’s really the point of the article, though: as always, prevention is the absolute best treatment.
Related Posts
Does Throwing Really Build “Arm Strength?”
What’s with all the Power Arms?
Archives:

