

Arm Care: Why Are We Still Talking About “Down and Back?”
Today’s guest post comes from Eric Schoenberg, the physical therapist at Cressey Sports Performance – Florida and a great resource to the entire CSP team. Enjoy! -EC
To get right to the heart of what I’m covering today, I think it’s best that we start with a video:
So, as you can infer, the reason we’re still talking about “down and back” is because we need to! Athletes are coming into the gym every week after multiple surgeries or drops in performance with postures and movement patterns that are faulty and easily correctible.

Obviously, the down and back concept is not the only reason for this, but the idea of driving our scapulae into maximal adduction (retraction), downward rotation, and depression is certainly something that we can control and improve upon.
To set the record straight, the only time an athlete should receive this cue is when their arms are by their side (Deadlifts, farmer’s walks, heavy dumbbell holds for lower body lifts). Once the humerus starts to move away from the side more than 20-30 degrees, the scapula needs to start moving in the appropriate direction to keep ball on socket congruency and reduce mechanical stress to the neighboring soft tissue structures (labrum, rotator cuff, neurovascular structures).
On the performance side of things, the “down and back” posture (scapular adduction, downward rotation, and depression) limit the ability to get the hand out in front or overhead. This has obvious implications in overhead athletes.
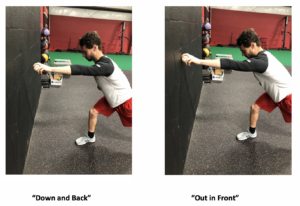
In the case of throwers, the difference in extension at ball release can vary by 3-4 inches depending on the position of the scapula. (as you can see in the comparison pics above and the video below).
When we don’t get full extension at ball release, any variety of downstream stresses can occur (aggressive elbow extension, lack of full pronation through the baseball) that result in increased injury risk and decreased performance.
As mentioned in the introduction video, we are bringing bad cues to good programming and it continues to result in faulty movement and injury. Even worse is when this “down and back” cue is brought into the rehabilitation setting and athletes that have already had surgery continue to experience symptoms similar to their pre-surgery presentation.
In conclusion, let’s continue to look at our cues and consider where the arm is in relation to the body when we decide to cue down and back. When the arms are by the side, then go ahead and cue the scaps down and back. However, when the arm is abducted to the side, overhead, layed back into ER, or out in front at ball release, we need to cue a degree of upward rotation and elevation to make sure the joint is aligned for success.
About the Author
Eric Schoenberg is a Physical Therapist and Strength Coach and the Owner of Diamond Physical Therapy located inside Cressey Sports Performance – Florida. Eric’s approach is to help athletes move more efficiently to reduce injury and improve performance. You can follow him on Twitter and Instagram at @csp_physicaltherapy, or email him at eric@diamondphystherapy.com.
Archives:

