

Shoulder Strategies and Hip Helpers: Part 1
I’ve spent the past week going through Tony Gentilcore and Dean Somerset’s awesome new resource, The Complete Shoulder and Hip Blueprint. With that in mind, Cressey Sports Performance staff member Tim Geromini and I pulled together ten solid takeaway points from the resource that we thought you’d like. Here are the first five, in no particular order…
1. Full scapular range of motion during push-ups often gets overlooked as a great “corrective.”
Tony did an excellent job of making this point during the shoulder portion of the seminar. Push-ups (when done properly) take take the scapula from retraction during the eccentric phase of the push-up to protraction and “wrapping around” the rib cage during the concentric phase. It is usually scapula protraction that is omitted, as many people only focus on straightening their arms to finish the push-up. This creates excessive glenohumeral (ball-on-socket) motion and insufficient scapulothoracic (shoulder blade on rib cage) movement.
Learning to “fill up” the upper back and get the shoulder blades to the arm pits can be a game changer for optimizing scapular control.
2. Your hip structure impacts your likelihood of surgical success.
Citing 2015 research from Fabricant et al, Dean noted that patients with retroverted hips had saw less improvement following surgery for femoroacetabular impingement (FAI) than those with anteverted hips.
This shouldn’t be surprising if you understand the implications of these hip presentations. Anteverted hips gives rise to more hip flexion and less hip extension, whereas retroverted hips will yield hips that do well with extension, but struggle getting into flexion.
FAI is a flexion-based pathology; bony overgrowth occurs because the femoral head (ball) bangs repeatedly into the acetabular rim (socket). It makes sense that a hip structure more conducive to allowing flexion would be less likely to re-develop these negative structural changes after a surgical intervention.
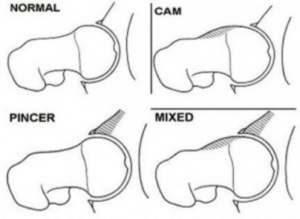
Source: Lavigne et al, 2004
That said, the big takeaway from this is that the more retroverted a hip is, the more conservative the rehabilitation ought to be – and the less aggressive that “patient” ought to be with squatting, etc. in the years that follow.
3. Don’t let a lack of a partner prevent you from doing rhythmic stabilization work.
The main function of the rotator cuff is to center the humeral head (ball) on the glenoid fossa (socket). Partner assisted rhythmic stabilization drills are fantastic in training this quality. Here’s an example:
However, if you don’t have a partner available to help, a nice substitute would be this simple exercise you can do with a band.
The pushing and pulling on the band with your free hand serves as form of distraction that will force the rotator cuff to resist. Of course, things like the Body Blade and Shoulder Tube can be options as well. Rhythmic stabilizations will always be the best option because they are less predictable, though.
4. Full exhalations can quickly enhance mobility – but only if you FORCEFULLY exhale.
A commonly overlooked limitation to mobility is alignment issues. As an example, if the pelvis is stuck in anterior tilt, the hip will be limited in internal rotation and flexion. As such, adding core stability (in this case, the ability to hold the pelvis in posterior tilt) can often quickly make changes to hip range of motion.
A great way to do this, as Dean notes, is to perform course stability exercises with full exhalations. When you exhale fully, the anterior core is engaged, as the rectus abdominis and external obliques, in particular, help to get air out. You can do this in various positions, but the most well-known are definitely prone and side plank positions with full exhale. It can’t just be a light exhale, though. You have to work very hard and blow out every last bit of air to get that cord engagement in order to really assess that positioning will change the range of motion.

We’ve used these strategies a lot in the past, but this video was a good reminder that we have to really push folks to get all that air out, especially if it’s the first time we’re cueing them to do so.
5. Make sure you’re getting motion in the right places during your thoracic spine extension work.
Improving thoracic spine extension in some people is an important part of improving overhead mobility. It’s not uncommon for many to grab a foam roller and haphazardly start leaning back in an attempt to do so. Unfortunately, many individuals perform their reps with incorrect technique; check out this video to learn more.
Speaking of learning more, I strongly encourage you to check out Tony and Dean’s excellent new resource, The Complete Shoulder and Hip Blueprint. It’s on sale for $60 off this week at an introductory discount; click here to learn more.

Archives:

