Today is the first day of games in Major League Baseball Spring Training, a day that's always circled on the calendars of just about anyone in the baseball world. We're excited to see all our pro players back on the field!
To celebrate, I've put my resource, Sturdy Shoulder Solutions, on sale for $40 off through this upcoming Sunday (3/7) at midnight.
This has been one of my most popular resources of all time, and it's particularly useful if you work with baseball players. Don't miss out on this great chance to pick it up at an excellent discount. Just head to www.SturdyShoulders.com and enter the coupon code ST2021 at checkout to get the discount.
Sign-up Today for our FREE Newsletter and receive a four-part video series on how to deadlift!
We're back with another edition of recommended reading, although this week will be much more about listening!
EC on the Stacked Podcast - I joined old friend Joe DiStefano for a podcast where we went into great detail on the unique nature of the shoulder joint - and how to keep it healthy in your training programs. You can listen to it right here, if you want:
EC on The Darren Woodson Show - Retired NFL player Darren Woodson and his crew have a great podcast that interviews successful folks from a variety of industries. It was an honor to join them:
I just saw that corner kicks and sliding in youth soccer are banned to prevent COVID spread. I hope that when normalcy returns, our elected officials pay as much attention to legislating against physical INACTIVITY/obesity as they have to legislating against physical ACTIVITY.
In this installment of Random Thoughts on Sports Performance Training, I want to hone in on shoulder stuff because, well, that's what I talk about a lot!
Let's get to the new content:
1. The neck is the easiest place to start with cleaning up shoulder movement.
I've written a lot in the past about how our arm care programs work proximal to distal, meaning that we focus on the center of the body before the extremities. Usually, the right proximal changes yield immediate distal improvements both via reducing protective tension and reducing stiffness in the muscles we're trying to "overpower" to create good movement. Usually, though, when it comes to proximal changes, folks look at the thoracic spine and rib cage only. In reality, the cervical spine ought to take precedence over both of them - particularly because all the nerve of the upper extremity originate from the brachial plexus, which ranges from C5 to T1.
Fortunately, while it might be anatomically correct, coaching optimal positioning in the neck is actually very simple in the context of weight training and arm care drills: get it to neutral and keep it there. In 99% of cases, that means getting people out of upper cervical extension, which fires up the levator scapulae (which competes against all the scapular upward rotation we want). Here's a video that walks you through what you need to know:
The thoracic spine and rib cage are sexy right now, but the cervical spine is an older, reliable option for cleaning up movement quickly in just about everyone.
2. Whenever possible, get core control integrated in your arm care drills.
I often come across arm care protocols that literally have athletes laying on a table for 30 minutes worth of "exercise." This not only leads to a disengaged athlete, but also overlooks the fact that the entire kinetic chain needs to be synced up to keep a shoulder healthy. We'll often use predominantly table-based exercises in month 1 to make sure athletes are picking up the technique in a controlled environment, but in almost all scenarios, these table drills are actually "fillers" between sets of strength training exercises that have the athletes up and around in the gym.
More importantly, after that first month, I try to make sure that at least half of our arm care exercises are done separate from the table. Maybe we do our horizontal abductions in a side bridge position, or integrate more bottoms-up carries or bear crawls for serratus activation. Perhaps the prone trap raises take place on a stability ball, or we shift to a TRX Y instead. Or, we could move the athlete to half-kneeling, split-stance, or in a rear-foot elevated position for their 90/90 external rotation holds.
Regardless of what we choose, the buy-in from athletes is definitely better - and just as importantly, the resulting training effect has a more specific carryover to sporting success.
3. Yet another study reminds us that GIRD is a measurement and not an actual pathology.
Glenohumeral internal rotation deficit (GIRD) was all the rage in the baseball sports medicine community for decades. Unfortunately, what many practitioners fail to appreciate is that GIRD can be a completely normal finding as long as an individual's total motion is symmetrical between throwing and non-throwing shoulders. We expect to see less internal rotation and more external rotation in a throwing shoulder because of retroverion in the throwing shoulder; the arc is just shifted. Here's a glimpse at what it looks like:
Anyway, we are now at a point in time where more and more research on GIRD is out there, and it's pretty resounding: it doesn't predict injury as well as we once thought. And, more importantly, the opposite seems to be true: a loss of external rotation (usually from a combination of less retroversion and soft tissue limitations) equates to a greater injury risk. We need to get more of the "GIRD? So What?" literature into the hands of doctors who aren't familiar with the latest research, as many are still making "GIRD" diagnoses when they really are just range-of-motion measurements. I delve into this in great detail in the Sturdy Shoulder Solutions product, but figured another study reiterating the point can't hurt. This one - Relationship Between Glenohumeral Internal Rotation Deficit and Medial Elbow Torque in High School Baseball Pitchers - just found that GIRD wasn't associated with medial elbow torque in high school pitchers.
It's time to move on from GIRD!
4. If you're about to have shoulder surgery (or any surgery), get your Vitamin D checked.
For years, we've known that having an adequate Vitamin D status was important for a myriad of biologic functions. Perhaps the most well known among observations on this front was a 2015 study of NFL players that demonstrated that players with inadequate preseason Vitamin D levels were more likely to have suffered a lower extremity or core muscle injury. In fact, the likelihood of a hamstrings injury was 3.61 higher in those with inadequate vitamin D levels! As such, it's become a big area of focus in the nutrition and supplementation world for athletes.
However, I've honesty never heard of an orthopedic surgeon looking at it for those who either have chronic pain or are about to undergo a surgical intervention to treat a structural defect. We need to change that, though. A recently published study, Preoperative Vitamin D Deficiency Is Associated With Higher Postoperative Complications in Arthroscopic Rotator Cuff Repair, should help in that goal, though. Patients with pre-operative Vitamin D deficiency were 1.54 times more likely to require a revision surgery and 1.16 times more likely to require manipulation under anesthesia to overcome post-op stiffness.
Clearly, Vitamin D has a huge link to soft tissue health, so don't overlook it!
Wrap-up
I'm a shoulder nerd and could ramble on all day on this stuff, but instead, I'll direct you to check out Sturdy Shoulder Solutions if you'd like to dig in deeper. You can learn more at www.SturdyShoulders.com.
Sign-up Today for our FREE Newsletter and receive a four-part video series on how to deadlift!
EC on the Lift the Bar Podcast - I joined Stuart Aitken on his podcast to chat about fitness industry success and building up career capital.
Gym Owner Musings: Installment 14 - My business partner, Pete Dupuis, always shares some good nuggets in these brain dumps. They're must-read for gym owners.
Top Tweet of the Week
In training, we can’t just think about the positions we achieve, but also 1️⃣ how we get to them and 2️⃣the direction and magnitude of the forces acting on us in these positions. https://t.co/fgnsz2ae4Jpic.twitter.com/05Lqu2TPlV
The subscapularis is the largest of the four rotator cuff muscles, but it might also be the most misunderstood. With that in mind, I thought I'd use today's video as a chance to bring you up to speed on it:
This video is an excerpt from my popular Sturdy Shoulder Solutions resource, which is on sale for 25% right now. For more information, head to www.SturdyShoulders.com and enter coupon code MLB2024.
Sign-up Today for our FREE Newsletter and receive a four-part video series on how to deadlift!
It's time for this month's installment of my random thoughts on sports performance training. In light of my ongoing sale on my Sturdy Shoulder Solutions resource, I thought I'd focus this edition on the shoulder.
1. If you want a healthy shoulder, getting tobacco products out of your life is a good place to start.
The research is pretty clear: smoking is a bad idea (and an independent risk factor) if you're looking to stay healthy from a musculoskeletal standpoint, or have a good outcome in rehabilitation (whether conservative or post-surgical) . Here's an excerpt from a recent study with an excellent review of the literature:
"Cigarette smoking adversely affects a variety of musculoskeletal conditions and procedures, including spinal fusion, fracture healing, surgical wound healing, tendon injury and knee ligament reconstruction. More recently, smoking has been suggested to negatively impact rotator cuff tear pathogenesis and healing. Tobacco smoke contains nicotine, a potent vasoconstrictor that can reduce the blood supply to the already relatively avascular rotator cuff insertion. Furthermore, carbon monoxide in smoke reduces the oxygen tension levels available for cellular metabolism. The combination of these toxins may lead to the development of attritional rotator cuff tears with a decreased capacity for healing."
Many times, we're looking for the best exercise, rehabilitation protocol, soft tissue treatment, or volume amounts - but we really ought to be looking at lifestyle factors.
With a large baseball readership on this site, the logical next question: are these harmful effects also noted with smokeless tobacco (i.e., dip/chew)? The research is somewhat sparse, as it's harder to study a younger, active population than a bunch of middle-aged post-operative rotator cuff patients. However, it's hard to believe that the aforementioned carbon monoxide implications would cause 100% of the issues and that the nicotine would serve as just an innocent bystander. So if you're looking to check every box in your quest to stay healthy, it's not a bad idea to lay off the dip.
And, if healthy tendons aren't enough to convince you, do yourself a favor and read this article by Curt Schilling.
2. The 1-arm, 1-leg landmine press isn't a mainstay in your training programs, but can be a perfect fit in a few circumstances.
This looks like kind of a wussy exercise, but I actually really like it in two circumstances.
a. It's awesome in a post-surgery period when you can't load like crazy, but still want folks to be challenged in their upper extremity progressions. The single-leg support creates a more unstable environment, which means that antagonist activity is higher and there is more work going to joint stability than actual movement. In other words, it makes pressing safer.
b. Once we get to the inseason period, it allows us to check two boxes with a single exercise: single-leg balance and upper body strength (plus serratus activation/scapular upward rotation).
I've written about it a lot in the past: core positioning has an incredibly important impact on shoulder function. Check out this study on how reducing anterior pelvic tilt increases lower trapezius activation during arm elevation and the return from the overhead position.
In my experience working with extension-rotation athletes (particularly baseball players), one of the biggest risk factors for shoulder injury is when the lower trapezius can't keep up with the latissimus dorsi. Just consider the attachment points of the lat in the picture below; as you can imagine, if you posteriorly tilt the pelvis, the lat is inhibited, making it easier for lower trap to get to work.
The lower trapezius is very important for providing posterior tilt (slight tipping back) of the scapula and assisting in upward rotation. These two functions are key for a pitcher to get the scapula in the correct position during the lay-back phase of throwing.
By contrast, the lat has more of a "gross" depression effect on the scapula; it pulls it down, but doesn't contribute to posterior tilting or upward rotation. This might help with an adult rotator cuff pain patient who has an aggressive scapular elevation (shrug) substitution pattern, but it's actually problematic for a thrower who is trying to get his scapula up and around the rib cage to make sure that the ball-on-socket congruency is "flush" when it really matters: the maximal external rotation position.
As such, you can say that the lat and lower trap "compete" for control of the scapula - and the lat has a big advantage because of its cross-sectional area and multiple attachment points. It's also much easier to train and strengthen - even if it's by accident. Upper body work in faulty core positioning (in this case, too much anterior pelvic tilt and the accompanying lumbar extension) shifts the balance to the lats.
We'll often hear throwers cued "down and back" during arm care drills. The intention - improving posterior tilt via lower trap activation - is admirable, but the outcome usually isn't what's desired. Unless athletes are actually put in a position of posterior tilt where they can actually feel the lower traps working, they don't get it. Instead, they pull further down into scapular depression, which feeds the lat-dominant strategy. This is why we teach almost all our throwers to differentiate between depression and posterior tilt early on in their training at Cressey Sports Performance.
If you're looking to learn more about how I assess, program, and coach at the shoulder, be sure to check out my popular resource, Sturdy Shoulder Solutions. Learn more at www.SturdyShoulders.com.
Sign-up Today for our FREE Newsletter and receive a four-part video series on how to deadlift!
My business partner, Shane Rye, once dropped an amazing one liner with respect to injuries that has stuck with me for years now:
[bctt tweet="You have to listen when it whispers instead of waiting for it to yell."]
The concept is simple: if you ignore minor aches and pains, they rarely just magically go away. Rather, they usually get magnified by volume and intensity and eventually reach a painful threshold where are more extensive intervention is required. The research actually supports this concept - but only if you know how to dig a bit deeper.
As an example, consider this Scandinavian study of patellar tendinopathy in junior basketball players. Researchers looked at 134 teenagers (268 total patellar tendons) and found that only 19 tendons presented clinically with symptoms. However, under ultrasound examination, 22% of the remainder of the group (who'd said they've never had patellar tendon pain) could be diagnosed with tendinopathy. In other words, "ultrasonographic tendon abnormality is 3 times as common as clinical symptoms."
Now, keep in mind that this study looked at teenagers, who are markedly less likely to have tendinopathy than older individuals. Just imagine if they'd done this study on a cohort of middle-aged men playing hoops at the local YMCA. The point is that whether you have symptoms or not, you likely have some changes in your tissues.
To be clear, this isn't particularly shocking to anyone who's looked at MRIs of asymptomatic individuals. We see loads of asymptomatic rotator cuff tears, spondylolysis (stress fractures), and torn labrums. And, I don't think we should just treat MRI findings when they aren't aligned with clinical symptoms. However, they do provide a reminder that we often have several issues that might just be waiting to reach a painful threshold if we aren't cognizant of our training volume and intensity - and our movement quality.
I call these potential problems "whispers." Maybe it's that Achilles tendon that's cranky first thing in the morning, but feels good after you warm it up. Or, it's that stiff neck you get after a few hours of working at the computer, but feels better after your spouse massages your upper trap. It could be the shoulder that bugs you only when you barbell bench press, but feels pretty good when you use dumbbells instead. These whispers are all premonitions of an imminent training disaster - so listen to them.
Maybe it's seeking out some extra manual therapy in a specific area. The solution could be looking at a more individualized warm-up to address these issues. It might even be that you strategically drop particular exercises from your program at various points during the year.
Above all else, though, it's about understanding that good training teaches your body how to spread stress over multiple joints. Instead of that cranky patellar tendon taking on 90% of the load on each landing, we work on hip and ankle mobility and strength so that it might only have to be 30%. Spreading out the stress ensures that one area won't ever hit the point of pain.
Understanding how to distribute stress mandates that you understand what quality movement actually looks like, though - and that's unfortunately where a lot of fitness professionals fall short. With that in mind, many of my products focus on the topics of assessment and corrective exercise, so they're good options for bringing these knowledge gaps up to speed. In particular, I'd recommend the following ones.
Sturdy Shoulder Solutions - this is my most up-to-date upper extremity resource, and it delves into everything from the neck, to thoracic spine, to scapular control. I discuss functional anatomy and key competencies you need for upper extremity health and high performance.
Functional Stability Training - this four-part series is a collaborative effort with physical therapist Mike Reinold, and we cover core, upper body, lower body, and optimizing movement. The components can be purchased individually or as the entire package (at a big discount).
Sign-up Today for our FREE Newsletter and receive a four-part video series on how to deadlift!
I wanted to introduce you to a new exercise we've been playing around with lately. I created the bent-over thoracic spine rotation with hip hinge because I was looking for a way for athletes to avoid compensatory movements as we worked on thoracic spine mobility in the standing position. Essentially, you'll often see folks with limited thoracic spine mobility move East-West with the hips or laterally flex through the spine as they try to find motion in spite of their limitations. By pushing the butt back to the wall, we effectively block off compensatory hip motion (and work on a better hip hinge pattern at the same time).
Key coaching points:
1. By having the eyes follow the hand, you get some cervical rotation to help things along.
2. Make sure the upper back is moving and you aren't just "hanging out" on the front of the shoulder. This is especially true in a throwing population who may have acquired anterior shoulder laxity.
3. We'll usually do eight reps per side. This can be included as a single set during a warm-up, or for multiple sets as fillers during a training session (we'll often plug it in between medicine ball sets).
4. This is a better option for those who have active range-of-motion limitations to thoracic spine rotation, as opposed to passive limitations. In the case of the passive limitations, athletes are better off with things like side-lying windmills, where they have assistance from gravity (instead of having to compete against it).
To learn more about how we assess, program, and coach around the thoracic spine (and entire shoulder girdle), be sure to check out Sturdy Shoulder Solutions.
Sign-up Today for our FREE Newsletter and receive a four-part video series on how to deadlift!
One of my biggest pet peeves is when all anterior shoulder pain is given a "blanket diagnosis" of biceps tendonitis. With that in mind, today, I've got a webinar excerpt from my Sturdy Shoulder Solutions resource (which is on sale for $40 off using coupon code APRIL22 right now) that delves into the topic in greater detail. Check it out:
For more information, check out www.SturdyShoulders.com. And, don't forget to enter coupon code APRIL22 to save $40 through Sunday at midnight!
Sign-up Today for our FREE Newsletter and receive a four-part video series on how to deadlift!
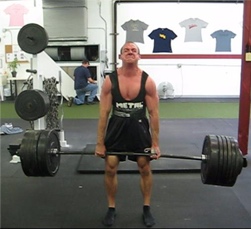
I see some of the lowest shoulders in history. This is a well-muscled guy who looks like his upper traps are non-existent because he sits in such significant scapular depression. Take note of the angle of his clavicles; normally, they should have an upslode from the sternoclavicular joint to the acromioclavicular joint, but in this case, they're actually downsloped. Wherever the scapula goes, the collarbone follows. In this presentation, expect to see tissue density in lats, subclavius, and scalenes (among other areas).
The most interesting discussion point, though, is what to do about that upper trap tightness. That tightness is protective tension: his body doing anything it possibly can to avoid dropping any lower into scapular depression. The upper traps are working to elevate the scapula against gravity all the time. If you give him a bunch of massage and stretching, it's like picking a scab; he'll feel better for 15 minutes, and then in rougher shape over the long haul. You never want to stretch out protective tension.
He'd had previous bouts of unsuccessful physical therapy, and while I had the benefit of hindsight here, it was clear that the unifying theme of these approaches was an emphasis on the one-size-fits-all "pull the shoulder blades down" cue that gets thrown around all too much and usually leaves this presentation in a tough spot while helping a lot of senior citizen rotator cuff pain cases. You can't one-size-fits-all cues because everyone moves differently.
We modified his training to avoid anything with heavy weights tugging the shoulders down (no deadlifts, walking lunges, farmer's walks, etc.) and instead trained the lower body with lots of front squat and goblet set-ups, plus sled work, glute-ham raises, and barbell supine bridges/hip thrusts. We cut back on lat dominant upper body work and instead chose drills like push-up variations and landmine presses that drove scapular upward rotation (and even prioritized elevation, which is borderline heresy in some rehab circles). We got his arms overhead more often during the warm-ups and integrated some manual therapy in the areas I noted earlier. I even encouraged him to do less unsupported sitting at work, too, because his upper traps were competing against gravity all the time (yes, there are actually times that standing desks make things worse).
Today, two weeks to the day after the evaluation, he's feeling significantly better - and training hard. Posture is the interaction of structure and function, and if you can't identify aberrant postures, you're simply guessing with how someone is going to respond to a given exercise.
Interested in learning more about what I look for when evaluating the upper extremity - and how my findings drive our programming and coaching cues? Check out Sturdy Shoulder Solutions (which is on sale for $50 off through Sunday at midnight) at www.SturdyShoulders.com.
Sign-up Today for our FREE Newsletter and receive a four-part video series on how to deadlift!